-
Overview
A raised level of thyroid hormone is called as hyperthyroidism. It has various causes but Graves’ disease is the most common cause. Hyperthyroidism can produce various symptoms. Thyroxine is a body chemical (hormone) made by the thyroid gland. It is carried around the body in the bloodstream. It helps to keep the body’s functions (the metabolism) working at the correct pace. Many cells and tissues in the body need thyroxine to keep them going correctly.
In an overactive thyroid gland, your thyroid gland makes too much thyroxine. The extra thyroxine causes many of your body’s functions to speed up. (In contrast, if you have hypothyroidism, you make too little thyroxine; this causes many of the body’s functions to slow down.) Thyrotoxicosis is a term that may be used by doctors instead of hyperthyroidism and implies high levels of thyroid hormone in the blood due to any cause; hyperthyroidism is the term reserved for situations where an overactive thyroid gland is the cause of the high level of thyroid hormones in the blood.
-
Causes
Many conditions can cause hyperthyroidism, including Graves’ disease, toxic adenoma, Plummer’s disease (toxic multinodular goiter) and thyroiditis. Your thyroid is a butterfly-shaped gland situated at the base of your neck, just below your Adam’s apple. Although it weighs less than an ounce, the thyroid gland has an enormous impact on your health. Every aspect of your metabolism is regulated by thyroid hormones.
Thyroxine hormone has two type, thyroxine (T-4) and triiodothyronine (T-3), that influence every cell in your body. They maintain the rate at which your body uses fats and carbohydrates, help control your body temperature, influence your heart rate, and help regulate the production of protein. Your thyroid also produces calcitonin, a hormone that helps regulate the amount of calcium in your blood.
Too much thyroxine (T-4) can be released due to many reasons, including:- Graves’ disease. It is an autoimmune disorder in which antibodies produced by your immune system stimulate your thyroid to produce too much T-4, is the most common cause of hyperthyroidism. Normally, your immune system uses antibodies to help protect against viruses, bacteria and other foreign substances that invade your body. In Graves’ disease, antibodies mistakenly attack your thyroid and occasionally attack the tissue behind your eyes (Graves’ ophthalmopathy) and the skin, often in your lower legs over the shins (Graves’ dermopathy). Scientists aren’t sure exactly what causes Graves’ disease, although several factors — including a genetic predisposition — are likely involved.
- Hyperfunctioning thyroid nodules (toxic adenoma, toxic multinodular goiter, Plummer’s disease). Hyperthyroidism of this form occurs when one or more adenomas of your thyroid produce too much T-4. An adenoma is a part of the gland that has walled itself off from the rest of the gland, forming noncancerous (benign) lumps that may cause an enlargement of the thyroid. Not all adenomas produce excess T-4, and doctors aren’t sure what causes some to begin producing too much hormone.
- Thyroiditis. Inflammation of thyroid gland for unknown reasons can result in hyperthyroidism. The inflammation can cause excess thyroid hormone stored in the gland to leak into your bloodstream. One rare type of thyroiditis, known as subacute thyroiditis, causes pain in the thyroid gland. Other types are painless and may sometimes occur after pregnancy (postpartum thyroiditis).
Risk factors
Talk to your doctor if any of your family members has hyperthyroidism particularly Graves’ disease, tends to run in families and is more common in women than in men.
-
Symptoms
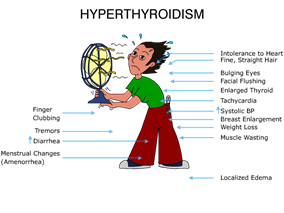
Many other disorders can be mimicked by hyperthyroidism, which may make it difficult for your doctor to diagnose. It can also cause a wide variety of signs and symptoms, including:
- Suddenly losing weight, even when your appetite and the amount and type of food you eat remain the same or even increase
- Accelerated heartbeat (tachycardia) — commonly more than 100 beats a minute — irregular heartbeat (arrhythmia) or pounding of your heart (palpitations)
- Increased appetite
- Nervousness, anxiety and irritability
- Tremor — usually a fine trembling in your hands and fingers
- Sweating
- Changes in menstrual patterns
- Increased sensitivity to heat
- Changes in bowel patterns, especially more frequent bowel movements
- An enlarged thyroid gland (goiter), which may appear as a swelling at the base of your neck
- Fatigue, muscle weakness
- Difficulty sleeping
- Skin thinning
- Fine, brittle hair
Aged people are more likely to have either no signs or symptoms or subtle ones, such as an increased heart rate, heat intolerance and a tendency to become tired during ordinary activities. Medications called beta blockers, which are used to treat high blood pressure and other conditions, can mask many of the signs of hyperthyroidism.
Graves’ ophthalmopathy
Rarely, Graves’ ophthalmopathy may affect your eyes, especially if you smoke. It is a rare disorder In this disorder, your eyeballs protrude beyond their normal protective orbits when the tissues and muscles behind your eyes swell. This pushes the eyeballs forward so far that they actually bulge out of their orbits. This can cause the front surface of your eyeballs to become very dry. Eye problems often improve without treatment.
Graves’ ophthalmopathy presents with:
- Protruding eyeballs
- Red or swollen eyes
- Excessive tearing or discomfort in one or both eyes
- Light sensitivity, blurry or double vision, inflammation, or reduced eye movement
-
Diagnosis
Hyperthyroidism can be diagnosed by a simple blood test. A normal blood test will also rule it out if symptoms suggest that it may be a possible diagnosis. One or both of the following may be measured in a blood sample:
- Thyroid-stimulating hormone (TSH). Pituitary manufactures this hormone. It is released into the bloodstream. It stimulates the thyroid gland to make thyroxine. If the level of thyroxine in the blood is high, then the pituitary releases less TSH. Therefore, a low level of TSH means that your thyroid gland is overactive and is making too much thyroxine.
- Thyroxine (T4). A high level of T4 confirms hyperthyroidism.
Borderline tests could be confusing. A normal T4 but with a low TSH also means future chances of developing hyperthyroidism. Other tests are sometimes done to clarify the situation and the cause. For example, another blood test that measures T3 is sometimes helpful and an ultrasound scan of the thyroid or a thyroid scan may be done if you have a nodular goitre.
In case of borderline results, one option is to repeat the tests a few weeks later, as sometimes borderline tests are due to another illness. Other tests may be done if a rare cause of hyperthyroidism is suspected.
Graves’ disease patients can undergo a blood test to detect specific autoantibodies which are commonly raised. However, these can also be raised in some people without Graves’ disease so this is not a specific test for Graves’ disease.
-
Complications
- Cardiovascular problems. Some of the most serious complications of hyperthyroidism involve the heart. These include a rapid heart rate, a heart rhythm disorder called atrial fibrillation and congestive heart failure — a condition in which your heart can’t circulate enough blood to meet your body’s needs. These complications generally are reversible with appropriate treatment.
- Bones becoming brittle and prone to fractures. Untreated hyperthyroidism can also lead to weak, brittle bones (osteoporosis). The strength of your bones depends, in part, on the amount of calcium and other minerals they contain. Too much thyroid hormone interferes with your body’s ability to incorporate calcium into your bones.
- Problems with eyes and vision. People with Graves’ ophthalmopathy develop eye problems, including bulging, red or swollen eyes, sensitivity to light, and blurring or double vision. Untreated, severe eye problems can lead to vision loss.
- Red, swollen skin. In rare cases, people with Graves’ disease develop Graves’ dermopathy, which affects the skin, causing redness and swelling, often on the shins and feet.
- Thyrotoxic crisis. Hyperthyroidism also places you at risk of thyrotoxic crisis — a sudden intensification of your symptoms, leading to a fever, a rapid pulse and even delirium. If this occurs, seek immediate medical care.
-
Treatments
Goal of treatment is to reduce your level of thyroxine to normal. Other problems, such as a large goitre (thyroid swelling) or associated eye problems, may also need treatment. Factors such as the underlying cause of the problem, your age and the size of any goitre are taken into account to decide on the best treatment plan.
Options for treatment are:Medicines
Drugs reduce the amount of thyroxine made by the overactive thyroid gland. The most common medicine used is carbimazole. Carbimazole does not affect the thyroxine which is already made and stored but reduces further production. Therefore, it may take 4 to 8 weeks of treatment for your thyroxine level to come down to normal. The dose of carbimazole needed to keep the thyroxine level normal varies from person to person. A high dose is usually given initially which is then reduced as your thyroxine levels come down.
It usually takes 12-18 months at first for carbimazole to fully act. After this, in about half of cases, the condition will have settled down and the carbimazole can be stopped. If the condition flares up again sometime in the future, a further course may be needed. However, in these cases an alternative treatment (for example, radioactive iodine) is often recommended. In about half of cases, carbimazole needs to be continued long-term to control symptoms. A different treatment may then be a better option if you do not want to take carbimazole long-term.Radioiodine
In this procedure, a drink is given to patient, or he is asked to swallow a capsule, which contains radioactive iodine. The main use of iodine in the body is to make thyroxine. Therefore, the radioactive iodine builds up in the thyroid gland. As the radioactivity is concentrated in the thyroid gland, it destroys some thyroid tissue which reduces the amount of thyroxine that you make. The dose of radioactivity to the rest of the body is very low and is not dangerous. However, it is not suitable if you are pregnant or breast-feeding. In addition, after treatment, women should not become pregnant for at least six months and men are advised not to father children for at least four months.
Thyroid replacement therapy
Drugs as well radioiodine can make your thyroxine level go too low. This needs replacement of thyroid. Not enough treatment means your level remains higher than normal. Regular blood tests are needed to check on the thyroxine level. One option is to take a high dose of carbimazole each day deliberately, or to receive a one-off high dose of radioiodine. This stops your thyroid gland making any thyroxine. You will then need to take a daily dose of thyroxine tablets to keep your blood level of thyroxine normal.
Surgery
In this, a part of your thyroid gland is removed surgically. It may be a good option if you have a large thyroid swelling (goitre) which is causing problems in your neck. If too much thyroid tissue is removed then you will be given thyroxine tablets to keep your thyroxine level normal. It is usually a safe operation. But, as with all operations, there is a small risk.
Beta-blocker medicines
These type of medications are prescribed in some people for a few weeks whilst the level of thyroxine is reduced gradually by one of the above treatments. Symptoms of tremor, palpitations, sweating, agitation and anxiety reduce with beta blocker medications.
External Links/References
http://www.mayoclinic.com/health/hyperthyroidism/DS00344
http://www.patient.co.uk/health/hyperthyroidism-overactive-thyroid
http://www.webmd.com/a-to-z-guides/hyperthyroidism-topic-overview
COPYRIGHT © 2023 ALL RIGHTS RESERVED | Developed By – OMX Technologies
For emergency cases (020) 30244100